The information in this section will help you to understand the fundamentals of diagnosing asthma in adults and young people aged 16+ in primary care. For children and young people under the age of 16 please visit this page.
This is not a substitute for completing an appropriate respiratory assessment module. For advice and support on choosing the right course for you, please see our training and development page.
What is asthma?
Asthma is a chronic respiratory condition associated with airway inflammation and hyper-responsiveness.
7.5 million people in the UK are living with asthma.
Symptoms include cough, wheeze, chest tightness, and shortness of breath.
Symptoms are variable - they can come and go.
Symptoms can be triggered by many factors such as exercise, allergen or irritant exposure, changes in weather and viral respiratory infections.
Symptoms may go by themselves or in response to medication, and may sometimes be absent for weeks or months at a time.
Studies estimate that approximately 30% of people with a diagnosis of asthma may not have asthma.
Asthma guidelines
There are currently 3 asthma guidelines in use in the UK
Although NICE have updated their guidance, QOF and other contracts and incentives may not yet be updated.
Asthma: diagnosis, monitoring and chronic asthma management (BTS, NICE, SIGN 2024)
GINA Report 2025, Global Strategy for Asthma Management and Prevention
All Wales Adult Asthma Management and Prescribing Guideline 2024
Diagnosing asthma in adults (over 16 years of age)
The diagnosis of asthma is like a jigsaw.
You need to fit all the pieces together to see the complete picture. It is important to remember that in asthma the symptoms, clinical examination findings and test results can vary over time and sometimes it’s necessary to re-examine patients and repeat tests when they have their symptoms.
There is no single diagnostic test for asthma. Diagnosis is based on a structured clinical assessment supported by objective tests that show airway inflammation or variable airflow obstruction.
Clinical assessment
Your first step should be to take a detailed clinical assessment.
|
Questions to ask your patient |
Why this question matters |
|---|---|
| Do you get a cough that comes and goes? | Asthma is a variable condition, with cough as a common symptom. A cough that is continuous is less likely to be asthma. |
| Do you get a tight feeling in your chest that makes it hard to breathe? | Chest tightness is a symptom of asthma and can be caused by untreated inflammation in the airways. |
| Do you get out of breath? What are you doing when this happens? How long does it last? | Breathlessness can be normal, especially during exercise, but is also a symptom of asthma. Understanding when your patient becomes breathless can help identify asthma triggers. |
| Is your chest or your breathing ever noisy? What does it sound like? | Avoid using the term 'wheeze' as this will be different for each person. Instead, ask them to describe any chest sounds or record them on their phone if they can. |
| Do you ever wake up in the night, or early in the morning with chest symptoms? | Night time or early morning symptoms are a sign of uncontrolled asthma. |
| Are there triggers for your chest symptoms? For example, allergens, exercise, pets, cold air, viral infections? | Symptoms in response to specific triggers make an asthma diagnosis more likely. |
| Can you breathe through your nose? Is it sometimes blocked or runny (rhinitis)? |
Breathing through the nose filters and humidifies air. Mouth breathing can trigger asthma symptoms as cold air or other allergens are breathed in. Rhinitis can be caused by allergies. |
| Do you get hayfever or eczema? Did you have either of these in childhood? | People with allergies or eczema are more likely to have asthma |
|
Did you have asthma as a child? Were you born prematurely? Does anyone else in the family have asthma? |
Childhood symptoms may not have been recorded as asthma but they may have been labelled as 'wheezy bronchitis' described as a 'chesty child' and these could suggest previous undiagnosed asthma symptoms. Low birth weight and prematurity are associated with asthma. |
| Do you have any other health problems such as lung cancer, COPD, post nasal drip, gastric reflux or anxiety? | All of these conditions can cause asthma like symptoms and happen in people with or without asthma. |
Most NHS IT systems allow you to make searches of your patient’s notes. This is quick and easy to do and can help you find information you can use to decide if someone is more or less likely to have asthma. Look for:
- Previous chest symptoms, including any chest infections
- A record of an HCP hearing a wheeze.
Look in the medications list. Has your patient ever been prescribed any
- Inhalers
- Oral steroids
- Antibiotics for chest symptoms?
Have they ever had a raised blood eosinophil count? Having a raised blood eosinophil count is a marker for asthma. However, there are other causes of raised eosinophils in the blood.
Chest auscultation
You should only listen to your patient’s chest if you are trained to do so. If your patient is symptomatic, you may hear an expiratory polyphonic (multiple pitches and tones on the out breath) wheeze over different areas of the lung. Remember, not all people with asthma wheeze.
Watch this video to hear lung sounds associated with asthma.
Safety note: this video is for information only and does not constitute training
Absence of wheeze does not rule out asthma as a diagnosis. This is because asthma is a variable condition, and your patient might not be symptomatic when you examine them.
Having completed and documented your clinical assessment, if you think your patient is likely to have asthma, code as suspected asthma.
Testing for asthma
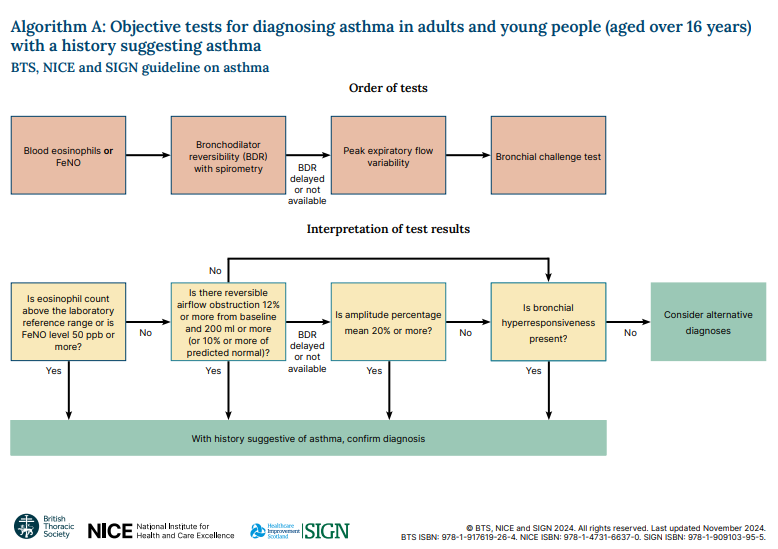
The first test should be blood eosinophils or FeNO (if available). If blood eosinophils are above the reference range or Feno is over 50ppb, then your diagnosis is confirmed.
Start your patient on treatment and code as asthma. Don’t forget to document the test results that you have used to confirm this diagnosis as these will provide a baseline for the patient’s future management. Include a validated questionnaire such as the Asthma Control Test.
Complete a personalised asthma action plan with your patient, using our guide how to complete an action plan. Save it to your patient’s notes and give them a copy.
Ideally, patients should have blood eosinophil testing and FeNO testing at their clinical assessment appointment but if this is not possible, you can start your patient on treatment and then bring them back for testing as soon as an appointment is available.
It’s important that starting treatment is not delayed in patients who are highly symptomatic, for example if they are having nighttime symptoms, or waking early in the morning because of cough, wheeze, chest tightness or shortness of breath. You may also need to consider using a short course of steroid tablets (prednisolone) if asthma symptoms are uncontrolled. For information about treating asthma flare ups and asthma attacks see here.
Further testing
If blood eosinophils or FeNO are below the levels above but you think your patient has asthma, you should perform bronchodilator reversibility using spirometry.
If the FEV1 increase is 12% or more and 200 ml or more from the pre-bronchodilator measurement, then your diagnosis is confirmed
If spirometry is not available in your area or there are long waits, you can start a peak flow diary. Asthma diagnosis can be confirmed if your patient's diurnal variability is 20% or more. Use our calculator tool to work out your patent's score.
If asthma is not confirmed by eosinophil count, FeNO, bronchodilator reversibility or PEF variability but you still think that it is a likely diagnosis, refer to secondary care for a bronchial challenge test.
The flowchart below explains the sequence of diagnostic tests for asthma and how to interpret them.