




This section will help you to understand asthma control in adults and the different types of treatments used to achieve it.
What is good asthma control?
Current asthma guidelines define good control as having:
• no symptoms
• no asthma attacks.
• no limitations on activity including exercise.
• no flare ups or exacerbations
• normal or near normal spirometry
Having symptoms at night time or waking up early in the morning with symptoms is a sign of poor control that needs urgent review.
Good control is achieved by dampening down the inflammation that is causing the asthma symptoms with inhaled corticosteroids (ICS).
Prescribing short-acting beta2 agonists (SABAs)
- Do not prescribe SABAs without also prescribing an ICS.
This is because studies show that only using a SABA to treat asthma is associated with a greater risk of fatal asthma attack - Newly diagnosed patients over 12 years of age should not be prescribed a SABA.
People with asthma often say they prefer their SABA to their ICS inhaler. This is because they can feel it working and it gives them instant symptom relief. So it’s important to explain to your patient that although their SABA makes them feel better immediately, it’s not actually treating the underlying problem, which is the inflammation in their airways.
SABA inhalers only treat symptoms. They do not treat the cause of the symptoms.
Starting treatment
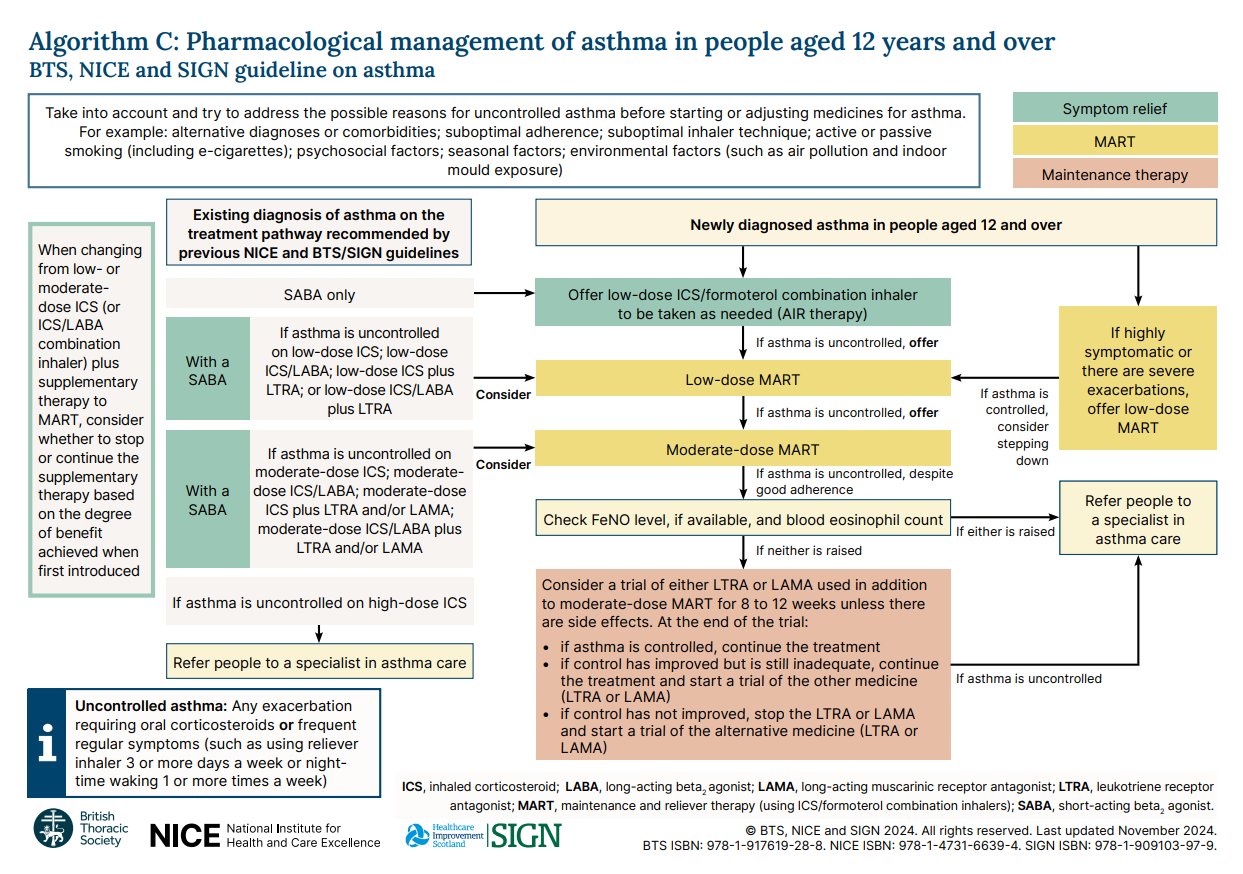
The BTS/SIGN/NICE asthma guidelines state that newly diagnosed patients should be prescribed a low dose ICS/Formoterol combination inhaler.
Why Formoterol?
Formoterol is a long acting bronchodilator (LABA). Formoterol is different from other LABAs because it has a rapid onset of action. It works quickly to open the airways but it lasts longer.
This means that an ICS-Formoterol inhaler can be used as a preventer AND a reliever. This helps your patient stay safe and reduce their risk of an asthma attack because:
• Every time they use their inhaler to treat symptoms, they’re also giving themselves a dose of ICS, which will help treat the underlying inflammation
• They only need to have one inhaler instead of two, which is especially helpful for people who pay for their prescriptions.
Anti Inflammatory Reliever (AIR) therapy
If your patients asthma symptoms are mild at the point of diagnosis, they can use their low dose ICS/Formoterol inhaler for symptom relief (PRN). This is called Anti Inflammatory Reliever (AIR) therapy.
Patients on AIR therapy should not be prescribed a SABA inhaler.
See here for A+LUK’s asthma action plan for AIR.
Maintenance And Reliever Therapy (MART)
If your patient’s asthma symptoms are uncontrolled, for example if they are waking at night or early in the morning with symptoms, or unable to do normal activities, then they can use their low dose ICS/Formoterol inhaler twice daily with additional inhalations as required (up to the maximum dose the inhaler is licensed for).
This is called Maintenance And Reliever Therapy (MART)
Patients on MART therapy should not be prescribed a SABA inhaler.
See here for A+LUK’s asthma action plan for MART
You might need to consider using a short course of steroid tablets (prednisolone) if asthma symptoms are highly uncontrolled. For information about treating asthma flare ups and asthma attacks see here.
Make sure your patient knows how to seek help if they get worse or are not improving.
Reviewing treatment
Review your patient after 8-12 weeks. Check their inhaler technique, assess their asthma control and you can also repeat their FeNO.
If they are fully controlled on a MART regime, you can consider stepping them down to an AIR regime. Ensure that they know they can increase it again if their symptoms get worse, for example, if they are needing to use their inhaler 3 times a week or more, or having night time symptoms.
If asthma is not fully controlled on low dose MART, you can increase the strength of their MART inhaler to a moderate dose.
Factors that can affect asthma control
If your patient is still showing signs of uncontrolled asthma, it's important to check the following factors before making any changes to their treatment.
Inhaler technique
Have they got good inhaler technique?
Is their inhaler device right for them?
It’s essential that patients are shown how to use their inhalers and are prescribed a device that is suitable for them. Click here for help on choosing the right inhaler device for your patient
Metered dose inhalers (MDIs) should always be used with a spacer.
Are they remembering to take their inhalers?
Suggesting your patient sets a reminder on their phone, downloads an app or keeps their inhaler next to their toothbrush might help them to remember to use it.
Exploring any worries or concerns about their medication will increase their understanding and adherence.
Triggers
Triggers are anything that causes asthma symptoms and vary from person to person. They often change over time. See here for more information on triggers
Are they smoking or exposed to smoke?
Offer smoking cessation support.
Click here to see Asthma + Lung UK's "How to stop smoking" leaflet
Are there any occupational exposures that are triggering their symptoms?
Are there any seasonal or environmental triggers, such as hayfever, pets, mould, air pollution?
Antihistamines are effective in treating allergies, seasonal or otherwise, that make asthma symptoms worse.
Gastric reflux
Do they have reflux?
People with asthma are more likely to get gastric reflux. Gastric reflux makes asthma symptoms worse as it causes irritation to the airways.
Although it’s not yet clear whether treating acid reflux improves asthma symptoms, there is some evidence to say it might improve them for some people.
Nasal symptoms
Can your patient breathe through their nose?
A runny nose (rhinitis) or nasal polyps can make asthma worse – it will be harder to breathe, and post-nasal drip (a feeling of mucus running down the back of the throat) may make your patient cough more.
Nasal steroids are effective in treating nasal symptoms.
Stepping up treatment
Once you are certain that all of the above have been assessed and treated, you can consider changing your patient’s asthma treatment.
For asthma that is not controlled on moderate-dose MART first of all check your patient’s FeNO (if available) and blood eosinophil levels. If either of these is raised, refer to secondary care.
If FeNO and eosinophil levels are not raised, you can give your patient either:
• an 8-12 week trial of a leukotriene receptor agonist (LTRA, also known as Montelukast). This must be taken alongside their moderate-dose MART.
Montelukast is taken at night time in tablet form. Ask your patient to keep a symptom diary during their trial of treatment. Make sure your patient knows to return if they have any side effects that are worrying them.
Or:
• an 8 to 12 week trial a long-acting muscarinic receptor antagonist (LAMA) alongside their moderate-dose MART.
If following this trial, asthma is well controlled, maintain the current treatment.
If control has improved but remains suboptimal, continue the current treatment and initiate a trial of the alternative medication (either LTRA or LAMA).
If there is no improvement in control, stop the current LTRA or LAMA and begin a trial with the other medication option (LTRA or LAMA).
At this point in your patient’s treatment, if you have checked technique, inhaler suitability, adherence and all the treatable traits above, you should refer your patient into secondary care for further testing and treatment.
This process is shown in the flowchart below.
Stepping down treatment
Once your patient's asthma is fully controlled over a 3 month period, consider stepping down .
Think about the following factors when you discuss this with your patient:
- How easy was it to get their asthma under control?
- Have previous attempts to step down resulted in a flare up of symptoms?
- Have they had a flare up or needed oral steroids (prednisolone) in the past 6 months? If so, delay stepping down for another 3 months8
- Are they under a respiratory specialist review or pregnant (only step-down if agreed with their specialist).
- Are there any seasonal considerations, for example, reviewing a patient outside of their hayfever season may not give an accurate picture of their asthma. In this case, reschedule stepdown review after season has ended.
- Are there any lifestyle considerations where stability is crucial, such as impending exams?
You can step your patient down from moderate to low dose MART, and then to AIR if appropriate. Don't forget to check your patient’s inhaler technique.
Update their asthma action plan and make sure they understand when and how to seek help if they get worse at any point.
Managing patients who are on SABA only, or who are not controlled on SABA+ ICS inhalers
It’s important to identify patients who are on SABAs alone, as they are at high risk of having uncontrolled or undertreated asthma, putting them at increased risk of asthma attacks and death. Most GP systems allow you to search for these patients.
Offer patients the opportunity to switch from an ICS + SABA regime at their annual reviews, or if you see them when their asthma is not controlled. Changes in medication need to be discussed with your patient to make sure they are happy to step down and understand why this is appropriate for them.
For more information about how to move your patient from an ICS+ SABA regime to AIR or MART, see the Primary Care Respiratory Society's guide.